
Table of Contents
- From Charity Care to Local Health Planning
- What a Community Health Needs Assessment Actually Measures
- How the Assessment Process Works: From Data Collection to Program Priorities
- Where Your Voice Enters the Assessment
- Tip: How to Read a CHNA Before a Community Meeting
- Key Takeaway: Local Data Becomes Local Care Only When It Is Connected to Action
- About the agfha Health Education Team
- Copyable Case: Turn a Parent Concern Into CHNA Input
Community Health Needs Assessments can look like dense public reports, but families should read them as something more practical: a map of what local organizations believe a community needs next. A strong CHNA can turn repeated neighborhood concerns into preventive care outreach, wellness education, screening events, referral navigation, and support programs that meet people closer to daily life.
From Charity Care to Local Health Planning
For a long time, many communities met health needs only after illness had already arrived. A family missed checkups, a chronic condition worsened, a hospital bill appeared, and then help entered the picture through charity care or emergency support.
Modern Community Health Needs Assessments grew out of a different question: what patterns can we document before families reach that point?

Over roughly the past decade or so, CHNA practice has moved toward recurring assessment cycles rather than one-time community reports. That shift matters. When a report tracks missed preventive care, transportation gaps, low screening access, or confusion about trusted health information, the conversation can move from general concern to local planning.
A CHNA is not a promise that every request will receive funding. It is a planning tool that connects local evidence, resident experience, and program decisions. At its best, it helps families see how a concern raised at a meeting can become a parenting class, a diabetes prevention workshop, a mobile screening day, or outreach in a neighborhood that has been easy to overlook.
What a Community Health Needs Assessment Actually Measures
A Community Health Needs Assessment is a structured review of health conditions, access to care, barriers, and resident priorities in a defined area. Plainly said: it asks what is getting in the way of family health, who is most affected, and what local resources could respond.
The most useful reports translate public health categories into issues families recognize. Look for sections that describe:
- Preventive care access: checkups, screenings, vaccinations, dental care, and nearby appointment options.
- Chronic disease concerns: diabetes, asthma, high blood pressure, heart disease, and the education needed to manage them.
- Maternal and child health: prenatal care, infant health, parenting supports, and school-linked resources.
- Transportation barriers: bus routes, clinic distance, ride availability, and the cost of getting to care.
- Food access: grocery availability, nutrition support, school meals, and food pantry connections.
- Behavioral health needs: stress, depression, substance use concerns, youth mental health, and referral pathways.
- Trusted health-information sources: the people, clinics, schools, faith groups, and community organizations families already turn to.
Good CHNAs pair numbers with people’s explanations. Local indicators may show rates of preventive screenings or disease burden, while listening sessions, surveys, interviews, and community partner observations explain what those numbers feel like in daily life. A transportation table can show distance. A parent can explain that the last bus leaves before the clinic’s evening appointment ends.
Note: A CHNA can reveal neighborhood-level patterns and service gaps. It does not diagnose an individual family or replace care from a clinician.
How the Assessment Process Works: From Data Collection to Program Priorities
The report is only one stop in the process. The work usually moves through a sequence, and each step changes what the final priorities can support.
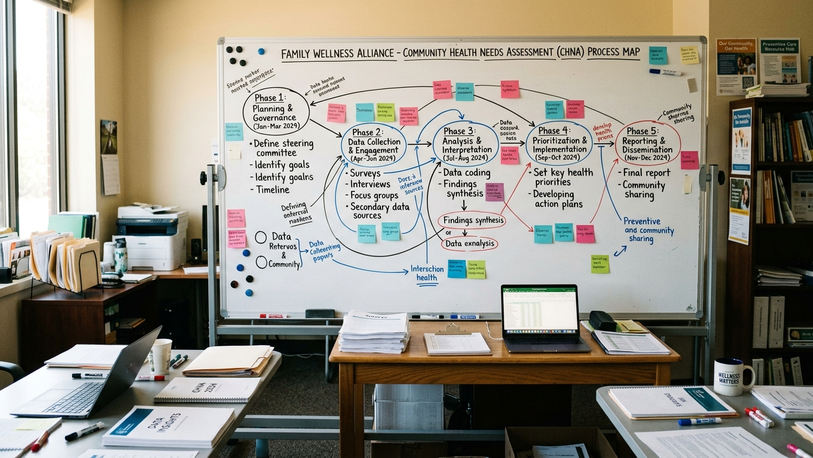
- Define the service area. The organization decides which counties, ZIP codes, neighborhoods, or patient communities the assessment covers.
- Gather local health data. Staff or partners review indicators tied to access, illness patterns, preventive care, and social barriers.
- Collect community input. Residents, families, service providers, schools, clinics, and community groups describe what they see on the ground.
- Identify recurring needs. The assessment team looks for issues that appear across multiple sources.
- Prioritize issues. Leaders weigh urgency, feasibility, community concern, and available resources.
- Publish findings. The CHNA becomes a public record of identified needs and priorities.
- Build an implementation plan. The organization decides which actions it will take, with what partners, and on what timeline.
Charitable hospital organizations subject to federal 501(r)(3) rules must conduct a CHNA at least once every three years, according to IRS guidance on Community Health Needs Assessments for charitable hospital organizations. Implementation plans are often adopted alongside or shortly after the assessment, though program rollout may wait for staffing, partner capacity, or a budget cycle.
That distinction prevents a common misunderstanding. A family may see transportation named as a top need and expect a van service right away. The actual response may be narrower: transportation navigation at a community health fair, appointment reminders through a school partner, or mobile screening events in one area first.
One practical boundary belongs here, not in fine print: agfha helps families interpret CHNA findings and prepare useful input, but it does not set or control local hospital or health-department funding decisions.
Where Your Voice Enters the Assessment
Resident input carries the most weight before priorities are finalized. After an implementation plan is adopted, comments may still matter, but they often feed the next cycle rather than the current program slate.
Families can usually enter the process through several doors:
- Community surveys
- Listening sessions
- Focus groups
- Town halls
- Advisory boards
- Conversations with community health workers
The strongest input is specific. Name the barrier. Say who it affects. Say when it happens, where it happens, and what would make care easier to use.
Consider one parent comment: Health education classes are offered at 11 a.m., but parents in our apartment complex work daytime shifts or pick up children from school. Evening classes at the library would be easier to attend. That comment gives planners a group, a schedule conflict, a location, and a workable adjustment.
A rural service area with one clinic and limited bus routes might rank transportation as the top barrier. A dense urban area with similar appointment data might rank clinic-hour mismatch higher because buses run often but appointments do not match work schedules. The program choice changes: one place may need ride coordination, while another may need evening appointment blocks.
Tip: How to Read a CHNA Before a Community Meeting
You do not need to read a long CHNA from cover to cover before speaking at a meeting. Some reports run well over a hundred pages, and the executive summary or priorities table often gives you enough to prepare.
Quick Tip: Bring one written example. A clear, one-page note beats a long list of unrelated concerns when meeting time is short.
Use this reading order
- Start with the service area. Confirm that your neighborhood, school district, town, or county is included.
- Read the top prioritized needs. Look for the issues the organization says it will address first.
- Check the community partners. Schools, food programs, faith groups, clinics, and family support organizations can show how close the plan is to daily life.
- Find the next steps. Look for the implementation plan, timeline, or named program areas.
Mark the match and the miss
As you read, mark two kinds of passages. First, note where the report matches your family’s experience. Second, mark where it misses something important. Both are useful at a meeting.
Then shape your comment in this order: problem, affected group, location, consequence, requested solution. For example: Parents at Lincoln Middle School miss well-child visits because the nearest clinic closes before work shifts end. This affects families without flexible jobs. A monthly evening clinic block or school-based reminder system would help.
Key Takeaway: Local Data Becomes Local Care Only When It Is Connected to Action
A completed CHNA is not the finish line. It is a decision tool.
Local data becomes local care when organizations connect findings to preventive care, wellness education, outreach, screening, and support programs. Clear resident input helps those organizations understand which barriers are urgent and which solutions are realistic enough to build.
Summary: A CHNA does not guarantee every requested program, but it creates a documented pathway for community needs to be considered and revisited in the next three-year cycle.
That record matters. If several families raise the same barrier before priorities are set, the issue becomes harder to dismiss as an isolated complaint. If a parent submits a detailed transportation concern two months after an implementation plan is adopted, the concern may not shape the current program slate, but it can still be logged for the next assessment cycle.
About the agfha Health Education Team
The agfha Health Education Team develops preventive care education, family wellness resources, and community support program guidance for families navigating local health systems. The team’s role in CHNA education is practical: help residents understand the reports, prepare specific input, and connect community concerns to the types of health programs that can respond.
This focus is educational and community-centered. It does not claim clinical, legal, or funding authority over local CHNA decisions.
Copyable Case: Turn a Parent Concern Into CHNA Input
Use this worked example if families in your area are missing preventive care because clinic hours and transportation do not line up.
Step 1: Write the concern in one sentence
Families in the north side apartment complexes are missing well-child checkups because the clinic closes before many parents get off work and the evening bus route does not stop near the clinic.
Step 2: Name who is affected
This affects parents working daytime or split shifts, school-age children who need annual checkups, and families without reliable cars.
Step 3: Say where and when it happens
The problem happens for families living near the north side apartment complexes, especially on weekdays after school and after standard work hours.
Step 4: Make a practical request
Ask the CHNA team to consider one of three options: one evening clinic block per month for preventive care visits, school-based appointment reminders sent home with students, or transportation navigation that helps families plan rides before appointments.
Step 5: Choose the submission route
Submit the comment through the CHNA survey if it is open. If a listening session is scheduled, bring the same note and read it aloud. If a community health worker is collecting feedback, hand them the written version so the details do not get lost.
Here is the copy-ready version: Families in the north side apartment complexes are missing well-child checkups because the clinic closes before many parents get off work and the evening bus route does not stop near the clinic. This affects parents working daytime or split shifts, school-age children, and families without reliable cars. The barrier happens on weekdays after school and after standard work hours. Please consider one evening clinic block per month, school-based appointment reminders, or transportation navigation for families scheduling preventive care visits. I am submitting this for the current CHNA because it affects multiple households and could be addressed through outreach, scheduling, or navigation support.








Add a Comment